Welcome to my site! I do tons of health research and created this blog to share what I've learned. I feel fortunate to have found affordable ways to stay healthy! Please note the recommendations on this site are not to be construed as MEDICAL advice. I am not a physician. Just a gal who found a bunch of things that happen to work brilliantly well for me. If you're very sick please see a physician. This site contains affiliate links for many things I've researched and used myself.
I have been trying to heal my own teeth for a few years. Recently I felt a lot of pain in a cracked / chipped tooth in which half the filling portion fell out. I have been determined to heal it myself, and am making this post to explain why I think it's possible. I will be posting pictures of my own progress, soon.
I am ordering two products that I will be posting further down the page. Tideglusib, plus an enzyme that eats up dental decay.
I realize I am taking a chance. I have no idea if this company is legit or not, but I do know that my late husband used to order stuff that worked (from a pharmacy in India) so I think it's worth taking a chance. I am going to just try out the smaller tube for now. It does help me to see that they are BBB accredited. They didn't seem to have any reviews, but at least there weren't any BAD ones that I could find.
Tideglusib (NP031112, NP-12) is an irreversible, non ATP-competitive GSK-3β inhibitor with IC50 of 60 nM in a cell-free assay; fails to inhibit kinases with a Cys homologous to Cys-199 located in the active site. Phase 2.
Selleck's Tideglusib has been cited by 22 publications
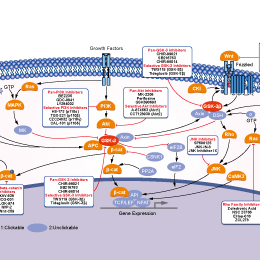
Notes: 2. For more details, such as half maximal inhibitory concentrations (IC50s) and working concentrations of each inhibitor, please click on the link of the inhibitor of interest. 3. "+" indicates inhibitory effect. Increased inhibition is marked by a higher "+" designation. 4. Orange "√" refers to compounds which do inhibitory effects on the related isoform, but without specific value.
Biological Activity
Description
Tideglusib (NP031112, NP-12) is an irreversible, non ATP-competitive GSK-3β inhibitor with IC50 of 60 nM in a cell-free assay; fails to inhibit kinases with a Cys homologous to Cys-199 located in the active site. Phase 2.
Tideglusib irreversibly inhibits GSK-3, reduces tau phosphorylation, and prevents apoptotic death in human neuroblastoma cells and murineprimary neurons. [1] Tideglusib (2.5 μM) inhibits glutamate-induced glial activation as evidenced by decreased TNF-α and COX-2 expression in rat primary astrocyte or microglial cultures. Tideglusib (2.5 μM) also exerts a potent neuroprotective effect on cortical neurons from glutamate-induced excitotoxicity as evidenced by significant reduction in the number of Annexin-V-positive cells in rat primary astrocyte or microglial cultures. [2]
Cell Data
Cell Lines
Assay Type
Concentration
Incubation Time
Formulation
Activity Description
PMID
SH-SY5Y
Function assay
10 uM
1 hrs
Inhibition of GSK-3beta in human SH-SY5Y cells assessed as reduction in amyloid beta (25 to 35) -induced toxicity at 10 uM pre-incubated for 1 hrs before amyloid beta (25 to 35) addition and measured after 72 hrs post Abeta25-35 addition by MTT assay
Inhibition of GSK-3beta in human SH-SY5Y cells assessed as reduction in amyloid beta (25 to 35) -induced toxicity at 30 uM pre-incubated for 1 hrs before amyloid beta (25 to 35) addition and measured after 72 hrs post Abeta25-35 addition by MTT assay
Tideglusib (50 mg/kg) injected into the adult male Wistar rats hippocampus dramatically reduces kainic acid-induced inflammation and has a neuroprotective effect in the damaged areas of the hippocampus. [2] Tideglusib (200 mg/kg, oral) results in lower levels of tau phosphorylation, decreased amyloid deposition and plaque-associated astrocytic proliferation, protection of neurons in the entorhinal cortex and CA1 hippocampal subfield against cell death, and prevention of memory deficits in APP/tau double transgenic mice. [3]
Add solvents to the product individually and in order(Data is from Selleck tests instead of citations): 4% DMSO+Corn Oil Click to purchase:Corn Oil For best results, use promptly after mixing.
2.5mg/mL
* Please note that Selleck tests the solubility of all compounds in-house, and the actual solubility may differ slightly from published values. This is normal and is due to slight batch-to-batch variations.
Chemical Information
Molecular Weight
334.39
Formula
C19H14N2O2S
CAS No.
865854-05-3
Storage
powder in solvent
Synonyms
NP031112, NP-12
Smiles
C1=CC=C(C=C1)CN2C(=O)N(SC2=O)C3=CC=CC4=CC=CC=C43
In vivo Formulation Calculator (Clear solution)
Step 1: Enter information below (Recommended: An additional animal making an allowance for loss during the experiment)
Answers to questions you may have can be found in the inhibitor handling instructions. Topics include how to prepare stock solutions, how to store inhibitors, and issues that need special attention for cell-based assays and animal experiments.
If you have any other enquiries, please leave a message.
Frequently Asked Questions
Question 1:
I want to deliver S2823 via i.p. injection, can you suggest one?
Answer:
This compound can be dissolved in 4% DMSO+corn oil at 2.5 mg/ml clearly. This is the highest concentration, since its solubility in DMSO is pretty low.
CHIR-99021 (CT99021) is a GSK-3α and GSK-3β inhibitor with IC50 of 10 nM and 6.7 nM, respectively. CHIR99201 does not exhibit cross-reactivity against cyclin-dependent kinases (CDKs) and shows a 350-fold selectivity toward GSK-3β compared to CDKs. CHIR99021 functions as a Wnt/β-catenin activator and induces autophagy.
LY2090314 is a potent GSK-3 inhibitor for GSK-3α/β with IC50 of 1.5 nM/0.9 nM; may improve the efficacy of platinum-based chemotherapy regimens. LY2090314 is highly selective towards GSK3 as demonstrated by its fold selectivity relative to a large panel of kinases.
TDZD-8 (NP 01139) is a non-ATP competitive GSK-3β inhibitor with IC50 of 2 μM; minimal inhibitory effect observed on CDK1, casein kinase II, PKA and PKC.
CHIR-99021 (CT99021) HCl is hydrochloride of CHIR-99021, which is a GSK-3α/β inhibitor with IC50 of 10 nM/6.7 nM; CHIR-99021 shows greater than 500-fold selectivity for GSK-3 versus its closest homologs Cdc2 and ERK2. CHIR-99021 is a potent pharmacological activators of the Wnt/beta-catenin signaling pathway. CHIR-99021 significantly rescues light-induced autophagy and augments GR, RORα and autophagy-related proteins.
TWS119 is a GSK-3β inhibitor with IC50 of 30 nM in a cell-free assay; capable of inducing neuronal differentiation and may be useful to stem cell biology. GSK-3β inhibition triggers autophagy.
SB216763 is a potent and selective GSK-3 inhibitor with IC50 of 34.3 nM for GSK-3α and equally effective at inhibiting human GSK-3β. SB216763 activates autophagy.
CHIR-98014 (CT98014) is a potent GSK-3α/β inhibitor with IC50 of 0.65 nM/0.58 nM in cell-free assays, with the ability to distinguish GSK-3 from its closest homologs Cdc2 and ERK2.
BIO (GSK-3 Inhibitor IX, 6-bromoindirubin-3-oxime, 6-Bromoindirubin-3'-oxime, MLS 2052) is a specific inhibitor of GSK-3 with IC50 of 5 nM for GSK-3α/β in a cell-free assay, shows >16-fold selectivity over CDK5, also a pan-JAK inhibitor with IC50 of 30 nM for Tyk2. BIO induces apoptosis in human melanoma cells.
Features:The first pharmacological agent shown to maintain self-renewal in human and mouse embryonic stem cells.
AR-A014418 (GSK-3β Inhibitor VIII) is an ATP-competitive, and selective GSK3β inhibitor with IC50 and Ki of 104 nM and 38 nM in cell-free assays, without significant inhibition on 26 other kinases tested.
I got the idea to take Alpha Lipoic acid to try to heal my tooth since I had learned how this stuff dramatically helps to repair a person's liver. It literally regenerates blood vessels. So I googled it to see if anyone else had used it, and this article popped up. Since I started taking it, it really helped!
Alpha-lipoic acid is a naturally occurring vitamin-like nutrient produced in small quantities within the body for catalyzing reactions and recycling beneficial materials such as vitamin C and E. It is key involving the nervous, cardiovascular, immune, and detoxification systems of the body. Alpha-lipoic acid can pass the blood/brain barrier and penetrate tissues with somewhat ease, allowing it to kill infection extremely effectively in nearly all parts of the body - in this case the head, mouth and teeth. Pain experienced during varying stages of tooth decay is nearly always a sign of infection, even if only mild and will cause some very severe side effects if not handled rather quickly.
A highly effective solution, particularly for those who cannot afford the ridiculous dental costs in the United States, is to keep infection away in the meantime using alpha-lipoic acid. Known as the "poor man's root canal" for it's effectiveness in removing infection and pain in dental decay situations, it should be considered one of the first choices in dealing with dental problems such as pain and infection alongside the standard practices of cleanliness via brushing and using a mouthwash containing 3% hydrogen peroxide - preferably homemade.
Dosage
A typical effective dosage of alpha-lipoic for acute pain and infection is approx. 50mg every 3-4 hours for an average sized adult. However some use 100mg of alpha-lipoic every 4-6 hours.
And while most bottles of alpha-lipoic acid come with their own ingestion instructions and amounts, the practice is to typically take a higher dose (as high as 300mg) only once or twice in a 24 hour period. This is not effective in the case of acute dental infection or pain, since a regular supply is more effective against infection. Investing in a pill cutter or crusher and splitting or cutting the pills into proper increments for taking periodically is an excellent idea.
If only mild soreness is experienced or one is just keeping maintenance over the body here or there, a larger dose of 150mg 1-3 times daily is a more proper amount.
Alpha-lipoic acid can be taken when one is experiencing pain or discomfort from infection. It should only take approximately 1-2 days to rid the body of infection and therefore most or even all pain. Some take alpha-lipoic acid as a dietary supplement for it's benefits and we recommend the ingestion of alpha-lipoic acid every once in a while as a form of body cleanse.
You can find a good source of alpha-lipoic acid here:
Alpha-Lipoic Acid - The Poor Man's Root Canal! Alpha-lipoic acid is a naturally occurring vitamin-like nutrient produced in small quantities within the...
Nov 8, 2020 — Conclusion alpha‐lipoic acid treatment provided therapeutic effects on the ... Root canal contamination or exposure to lipopolysaccharide ...
by O Molven · 2002 · Cited by 159 — Endodontics Periapical changes following root-canal treatment observed ... blind controlled study of alpha-lipoic acid (thioctic acid) therapy.
Address the root cause of oral health issues today. ... They told me that one tooth is dead and they wanted to do a root canal. I refused. I'm in to ... And recently I started taking Alpha Lipoic Acid 600mg and that helped even more. Any other ...
by S Akman · 2013 · Cited by 64 — This study shows that ALA and Vit-C treatment provides therapeutic effects on inhibition of alveolar bone resorption and periodontal tissue destruction.
Aim To investigate the possible therapeutic effects of alpha‐lipoic acid (ALA) in a model of chronic apical periodontitis in rats by analysing biochemical, histopathological and micro‐CT parameters. Methodology The study was approved by the Animal Ethics Committee of the Near East University. Thirty‐two Wistar rats were divided into four groups of eight rats each: Control Group; ALA Group; AP Group; AP + ALA Group. In the AP and AP + ALA groups, the pulp chambers of the mandibular first molars were surgically exposed and were left open to the oral environment for 4‐weeks to allow the establishment of periapical lesions. The rats in the Control and AP groups were treated intraperitoneally with saline solution (with a daily dose of 100 mg kg⁻¹, for 28 days after periapical lesion induction). The rats in the ALA and AP + ALA groups were treated intraperitoneally with ALA (with a daily dose of 100 mg kg⁻¹, for 28 days after periapical lesion induction). After decapitation, the trunk blood was collected for the assessment of biochemical parameters. The mandibles were surgically removed and dissected for histopathologic analysis and further scanned with micro‐CT. Groups of data were compared with a two‐way analysis of variance (two‐way anova) followed by Sidak's multiple comparison tests. Values of P < 0.05 were regarded as significant. Results TNF‐α, IL‐1β, MMP‐1, MMP‐2 levels were significantly lower in AP + ALA group compared with AP group (P < 0.05). There was a significant difference between the AP and AP + ALA groups according to assessment of the inflammatory scores (P < 0.05). The periapical inflammatory infiltrates were significantly more severe (P < 0.05) in the AP group. The AP + ALA group exhibited lower values both in terms of surface area and volume of resorption cavities than the AP group and this difference was significant (P < 0.05). Conclusion alpha‐lipoic acid treatment provided therapeutic effects on the inhibition of periapical bone loss.